Gastric volvulus


Gastric volvulus

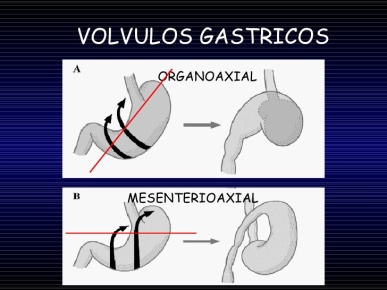
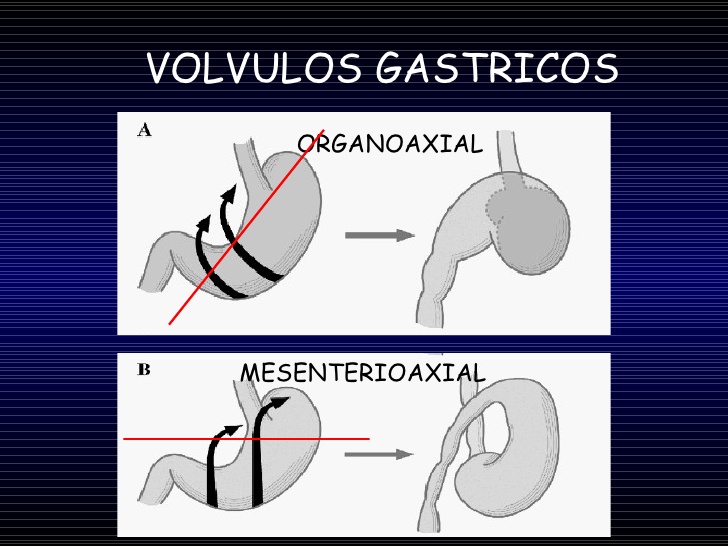
- 3 types: organoaxial (more common, associated with diaphragmatic defects), mesenteroaxial (more common in paediatric population, less associated with diaphragmatic defects, more severe obstruction), mixed
- Borchadt’s triad: severe epigastric pain, retching without vomiting and inability to pass NG tube
- High risk of gastric ischemia and perforation.

Diagnosis
- UGI series
- CT
– Early CT of the abdomen and pelvis is recommended when gastric volvulus is suspected; it will aid in distinguishing this from hiatal hernia. - Gastric wall pneumatosis and free fluid in hernia sac = impendic rupture
Management
- Non-surgical (no clinical and radiographic evidence of gastric strangulation):
– Nasogastric or endoscopic decompression with percutaneous gastrostomy may be considered, high recurrence rate as the defect persists and stomach has not been reduced to its anatomical position - In stable patients, the stomach is detorsed, and then laparoscopy or laparotomy to repair the diaphragmatic defect with gastropexy
- In unstable patients, partial gastrectomy is considered.
– If gastric necrosis happens, often in fundus -> sleeve gastrectomy can be done
