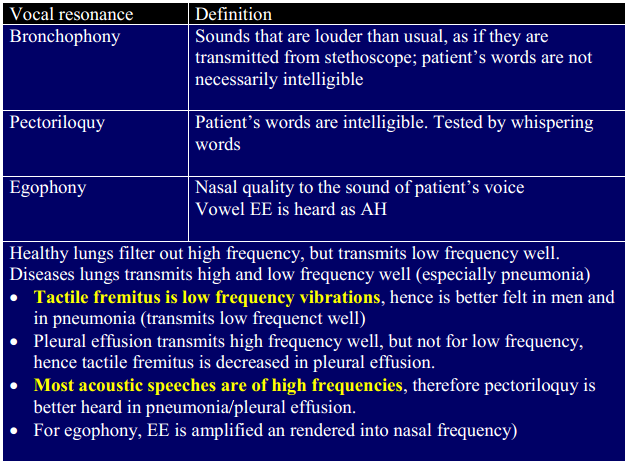
Saying “ninety-nine” while palpating the chest wall
More prominent in men due to lower pitched voices.
ONLY ASYMMETRICAL FINDING IS SIGNIFICANT.
Percussion
3 types
Comparative
Topographical: used to delineate border of heart, liver and diaphragmatic excursions.
Auscultatory
Auscultatory percussion
Pleural effusion: stethoscope is placed below 12th rib. Percussion is done from posterior chest from apex to base.
– At some point, the dull sound will change to a clearer one as it approaches the stethoscope. If this happens above 12th rib, it indicates pleural effusion.
Another version is by listening over the back of chest while tapping over the manubrium.
– Clinician should hear identical sounds in two sides of chest. A decreased intensity indicates ipsilateral disease on that side
Percussion sounds
Resonance
– Special types of resonance: Skodaic’s, amphoric
Dullness
Tympanic
Skodaic resonance:
Resonance heard above the pleural effusion.
Why? Nobody knows
Amphoric resonance
Flicking the tense cheek while holding the mouth open mimics the sound
Indicates presence of cavities.
Grocco’s triangle
A small triangle of dullness at posterior chest contralateral to side of effusion
Kronig isthmus
Narrow area of resonance between the dullness of neck and shoulder muscles.
If this resonance is lost, it indicates apical lung diseases.
Pathogenesis
Topographic percussion theory
– The characteristics of the underlying organs determine the type of the sounds heard.
Cage resonance theory (the chest wall is the cage, and how it resonates affects the percussion)
– The type of sounds are also affected by the chest wall and the strength of the stroke.
Cage resonance theory maybe more accurate:
External pressure on the chest dampens the percussion notes.
Liver span is SMALLERwhen percussing with stronger stroke. – Stronger stroke produces more vibrations and therefore more resonance.
– If according to topographic percussion theory (stronger strokes lead to deeper penetration), the liver span should have been larger.
Auscultatory percussion
Possibly sound transmission circumferentially in chest wall rather than through the lungs
Evidences: – Heart is not detected.If the sound is transmitted through the lung, some dullness should have been heard in left side of the chest – Sounds intensity changes during Valsava maneuver which tenses the chest wall.
– Sound intensity recorded when the patient breathes room air and a mixture of oxygen and helium is the same (different gases should have different density and this affects the sound intensity).
So what’s good?
Only asymmetrical dullness/hyperresonance using comparative percussion maybe ok to detect pulmonary pathologies.
Auscultatory percussion is also very specific for detecting pleural effusion.
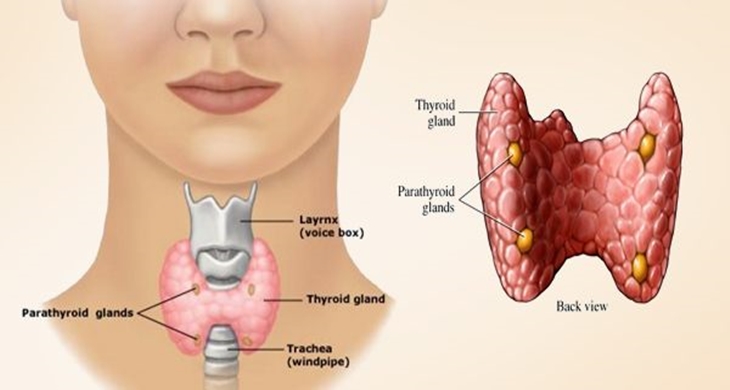
Landmarks: laryngeal prominence (adam’s apple) of thyroid cartilage and cricoid cartilage which lies below it
Isthmus of thyroid normally lies just below the cricoid cartilage
High vs low lying thyroid
– If distance between laryngeal prominence and the suprasternal notch is far (eg 10cm), the thyroid gland maybe high lying (pseudogoiter)
– If laryngeal prominence is close to suprasternal notch (<5cm), the thyroid gland is low lying (and located retrosternally). Palpation maybe impossible.
Inspection of thyroid gland
See from the side. The line between cricoid prominence and suprasternal notch (where the thyroid gland is located) is a straight line.
If it is bowed, consider goiter
Palpation
An easier way to palpate thyroid gland
What do we palpate?
Size
Consistency (hard or soft)
Nodular
Tenderness
The key to know that what we palpate is thyroid gland is
It moves during swallowing, and then hesitate a while before returning. As thyroid gland and tracheal is connected by ligaments.
If it does not move during sallowing or does not hesitate before returning to its original position, it is likely not thyroid gland.
Cervical goiter
Estimation of size
Rule of thumb: lateral lobe is enlarged if it is larger than distal phalanx of the patient’s thumb
WHO grading
Retrosternal goiter
May cause TOS, SVC syndrome and compression of trachea and esophagus
TOS (thoracic outlet syndrome):
– Compression of brachial plexus: pain in the multiple myotomes in UE
– Compression of subclavian vein: UE venous thrombosis (Paget-Schroetter syndrome)
Compression of trachea and esophagus: dyspnea, stridor, dysphagia
Thyroglossal cyst
Cystic swellings of thyroglossal duct , an epithelium lined remnant marking the descent of thyroid tissue from the base of tongue to its final location
Midline neck mass
Characteristic sign is upward movement when the patient protrudes the tongue
Delphian node
Prelaryngeal lymph node
Named Delphian because it is the first one exposed during surgery and its appearance often foretells what the surgeon will find in thyroid.
Radiologically, it is situated in lymph node level VI
If it’s palpable, it is usually enlarged – suspect malignancy or Hashimoto’s thyroidits
Features
– Skin: dry, cold, puffy skin
– Achlles reflex: delayed reflex due to prolonged contraction & relaxation
– Hypothyroid speech: slow, deep and nasal (as if patient has a cold)
Billewicz Diagnostic Index for hypothyroidism
>30 has a high likelihood of hypothyroidism
Graves disease
Triad of prominent eyes + goiter + tachycardia
Auscultation in thyroid gland can often ellicit bruit (in 70% of patents)
Eye findings:
Lid lag: von Graefe sign
– ask patient to look down, the upper eyelid “lags” behind
Lid retraction: Dalrymple’s sign
– ask patient to look straight, white sclera is seen between the limbus and the lid margin; usually the lid margin rests just below the corneal limbus
Graves opthalmopathy
– NO SPECS
– Consider if patient with Graves disease complain of gritty sensation in the eyes or diplopia
CV findings:
– Loud S1
– Tachycardia
– Means Lerman scratch (systolic rub resembling scratching near the left 2nd ICS)
Skin findings:
– Moist (due to increased sweating) and warm
– Pretibial myxoedema
Neuromuscular findings
– Fatigue & weakness
– Fine tremor due to sympathetic overflow
– Brisk ankle reflexes
** Other ddx of lid retraction
Facial palsy: unilateral weakness of orbicularis oculi–> levator palpebrae is no longer being opposed
Unilateral ptosis: attempts to elevate the weakened lid causes excessive neural signals which end up elevating another lid
Previous eyelid surgeru
More eponyms?
Von Graefe: lid lag (We look down in Grief !)
Darylrmple sign: lid retraction (DaryLRmple)
Joffroy sign: lack of forehead wrinkling (FF resembling wrinkling)
Stellwag sign: staring look (Stellwag for Staring)
Moebius sign: Poor convergence (Merging Of EyeBalls Is UnSuccessful)
Wayne Diagnostic Index for hyperthyroidism >20 points have a high likelihood for hyperthyroidism
Note: BOTH hypo and hyperthyroidism cause amenorrhea !
Hypothyroidism: increased TRH causes increased prolactin production which blocks GnRH
Hyperthyroidis: multiple mechanisms, but likely linked to high SHBG which leads to high ratio of bound estradiol. Only free estradiol can induce a LH peak.
Mnemonic for THYROID disorders: NEVER FORGET THEM AGAIN !
THYROIDISM
Tremor (in hyper)
Heart Rate
Yawn (fatigue in both)
Reflexes (brisk or delayed)
Oligomenorrhea
Intolerance to temperature (heat or cold)
Diarrhea (or constipation)
Increased or decreased appetitie
Skin (cool,dry and puffy or moist and warm skin)
Myxoedema (facial puffiness in hypothyroidism, pretibial myxoedema)
Reference:
Steven McGee. Evidence Based Physical Diagnosis. Pg 250-276
Especially poorly controlled hypertensive patients.
A “sudden” NORMAL BP could mean compensated shock
Even for normal person, do not exclude compensated shock because BP is “normal” !
Diabetes
Osmotic diuresis paves the way for dehydration !!
Pregnant women
Lower baseline Hct, so Hct in dehydrated pregnant patients maybe magically “normal” !
Due to progestogen induced vasodilation, baseline DBP is lower, especially in 2nd trimester. The pulse pressure may not even get narrow to be in shock !
Mentioned in NICE 2009 guideline for T2DM but not in 2015.
Insulin secretagogue, especially increases its secretion in response to glucose (first phase insulin release). – Used in patients with unpredictable meal time.
– Good to tackle postprandial hyperglycemia (mild increase in fasting glucose level but disproportionately high A1C)
Short duration of action (achieves peak plasma level in 1 hr & producing a rapid insulin-releasing effect that lasts for 3 hrs ) and hepatically excreted (T1/2 = 1 hr)
– Can be used in renally-impaired patients
– Lesser hypoglycemia (as it is short acting and increases insulin secretion IN RESPONSE to glucose, unlike sulfonylureas)
Rational of combination therapy
NICE suggests metformin + sulfonylurea or pioglitazone or DPP4i
Common threshold to initiate combination therapy is when A1C >8%.
With time, not only insulin resistance, there is loss of B-cell function as well(to abou 25% in 6 years).
Primary objective is to tackle the problems of insulin resistance + deficiency.
– Metformin: insulin sensitizer
– Pioglitazone: insulin sensitizer
– Sulfonylurea: insulin secretagogue
– DPP4i: GLP-1 based (increases insulin secretion)
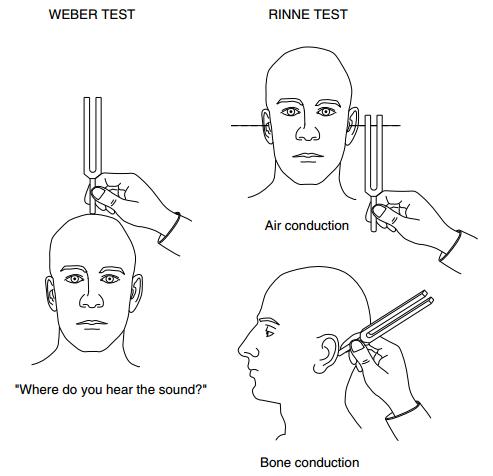
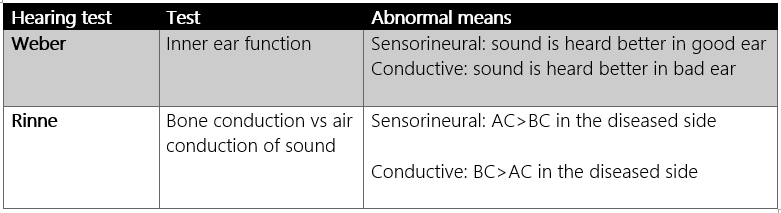
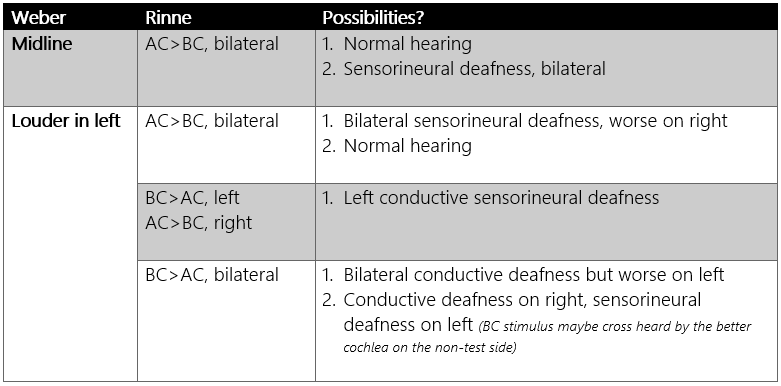
Lateralization in Weber test
– Sensorineuralloss: to good ear (= CONTRALATERAL ear is damaged)
– Conductiveloss: to bad ear (= IPSILATERAL ear is damaged)
Rinne test
– BC>AC in conductive loss
– AC>BC in sensorineural loss
Reference:
Steven McGee. Evidence Based Physical Diagnosis. Pg 242-249