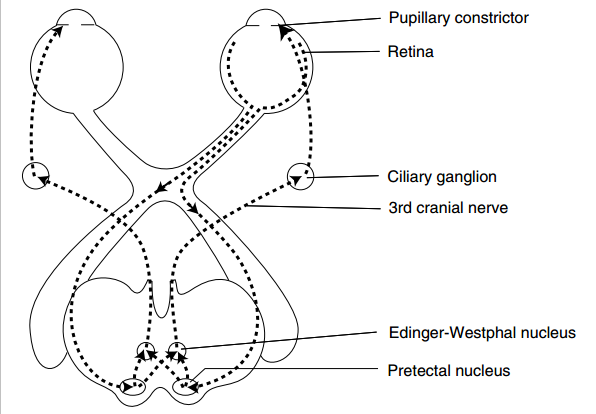
Normal light reflex pathway
Hippus
- In steady illumination, normal pupil is continuously dilating and contracting. This is called hippus (pupil undulation).
Simple anicosoria
- Definition of anicosoria: >0.5mm different in dize of the left and right pupil
- Simple = cannot be atributed to secondary causes eg trauma, drugs etc, occurs in up to 40% of healthy persons
Normal light reflex
- Direct and consensual reaction
– Direct: ipsilateral pupillary constriction
– Consensual: contralateral pupillary constriction - Clinical significance: Anicosoria is
– absent in disorders of the optic nerve or retina (i.e afferent connections)
– present in asymmetric disease of the iris, sympathetic nerve or oculomotor nerve
(i.e efferent connections)
Near synkinesis reaction: when a person focuses on near object:
- Constriction
- Convergence
- Accomodation
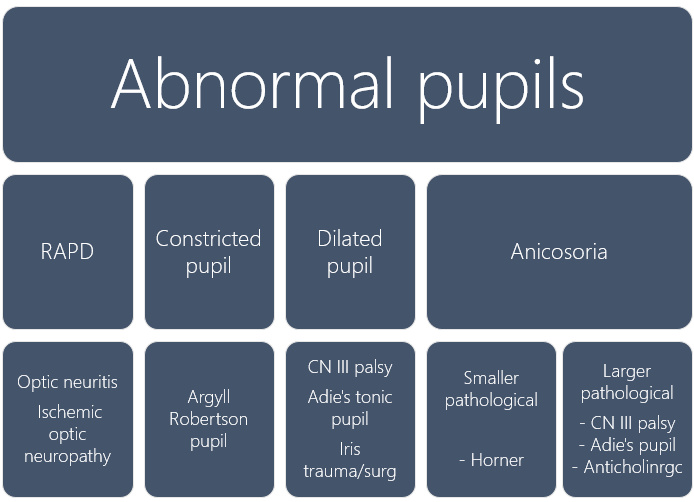
Abnormal pupils
- RAPD (Marcus-Gunn pupil)
- Argyll Robertson pupils
- Oval (dilated pupils)
- Anicosoria
Relative afferent pupil defect (Marcus-Gunn pupil)
- Detected by swinging flashlight test
- Finding: detection of absence of direct or consensual response of the pupil
- Clinical significance:
– Optic nerve disease (eg optic neuritis, ischemic optic neuropathy)
** Cataracts DO NOT cause RAPD as the retina behind it is intact.
Argyll-Robertson pupils
- Mnemonic: ARP PRA
– Accomodation reflex present, pupillary reflex absent
– Bilateral SMALL PUPILS
– Constriction & redilation of pupils are brisk - Historically due to 3rd stage of syphilis
- Differential diagnosis of light-near dissociation
– Adie’s tonic pupil
– Parinaud syndrome (dorsal midbrain syndrome)
– Aberrant regeneration of third nerve - Parinaud syndrome (dorsal midbrain syndrome)
– Ddx: young: pinealoma; middle age lady: MS; old: basilar artery stroke
– CLUES: Convergence-retraction nystagmus, Light near dissociation, Upward deviation, Eyelid retraction, Setting sun sign
Oval pupil
- Third nerve palsy from brain herniation
- Adie’s tonic pupil
- Previus surgery or trauma to iris (pupillary constrictor)
Pathological anicosoria
- Which side is abnormal?
– Swing a flashlight to the dilated eye. If the ipsilateral eye does not constrict, the pupillary constrictor at the side is abnormal. If it does constrict, the contralateral (smaller) eye is abnormal. - 2 questions
i) Is there full 3rd nerve palsy?
ii) Neurological findings?
Smaller eye is the problem:
- Horner syndrome
- Simple anicosoria
Bigger eye is the problem:
- 3rd nerve palsy from brain herniation or Hutchinson pupil (if comatose) or PCA aneurysm (if not comatose)
– Ptosis and pupil will appear “down and out” in 3rd nerve compression - Adie’s tonic pupil (respond to pilocarpine)
- Anticholinergic mydriasis (does not respond to pilocarpine)
Adie’s tonic pupil
- Unilateral LARGE PUPIL
- Tonic = SLOW constriction and redilation in respponse to near vision
- Light reflex is absent
- Adie’s syndrome: tonic pupil + hyperhidrosis + areflexia
- Due to injury to the ciliary ganglion and postganglionic fibers (eg viral infection)
– The fibers destined to ciliary body instead aberrantly re-innervate pupillary constrictor. Hence, the loss of light reflex.
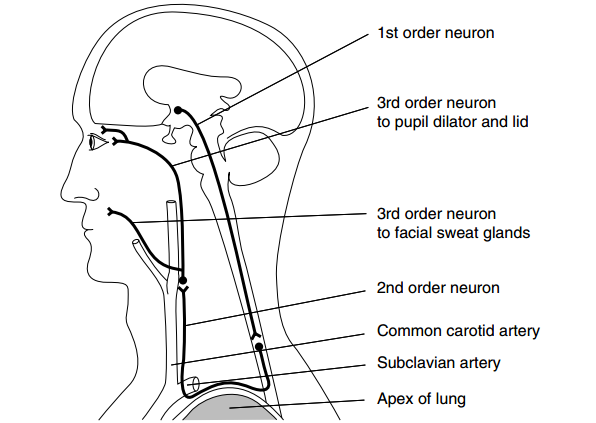
Horner syndrome
- Ptosis, miosis, anhidrosis, enophthalmos
- Presence or absence of anhidrosis may indicate level of lesion
– 1st order (preganglionic eg stroke): anhidrosis present in face and trunk
– 2nd order (ganglionic eg Pancoast syndrome, cervical rib): anhidrosis only in face
– 3rd order (postganglionic eg ICA dissection): no facial anhidrosis
– This is because neurons to facial sweat glands are located in ECA
– However, this was found to be limited in utility (not significant LR)
Summary
Reference:
Steven McGee. Evidence based Physical Diagnosis. Pg 209-233
